KRAS Mutation Panel
KRAS overview:
- The RAS genes are highly homologous but functionally distinct[1]
- RAS proteins are central mediators for the downstream of growth factor receptor signaling and therefore are critical for cell proliferation, survival, and differentiation.
- RAS can activate several downstream effectors, including the PI3K-AKT-mTOR pathway, which is involved in cell survival, and the RAS-RAF-MEK-ERK pathway, which are involved in cell proliferation.
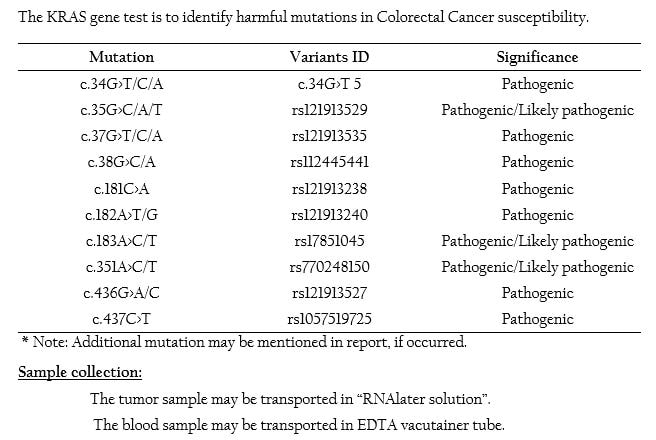
- The KRAS gene encodes one of the proteins in the Epidermal Growth Factor Receptor (EGFR) signaling pathway that is critical in the development and progression of cancer.
- Activating mutations within the RAS gene result in constitutive activation of the RAS GTPase, even in the absence of growth factor signaling. The result is a sustained proliferation signal within the cell.
- Specific RAS genes are recurrently mutated in different malignancies. KRAS mutations are particularly common in colon cancer, lung cancer, and pancreatic cancer[2]
- KRAS mutations are more commonly observed in Cecal Cancers than Colorectal Cancers located in any other places ascending from colon to rectum[3&4].
- High rates of Somatic and Germline KRAS mutations are found in colorectal cancer[5].
- An estimation of 50% of the CRC patient tumors include an oncogenic KRAS mutation, in an addition ~6% of colorectal tumors contain mutations in NRAS or HRAS[6&7].
- KRAS mutation frequency is found to be significantly higher as compared to colon cancers and interestingly this genetic alteration showed a strong association with female sex[8].
- Furthermore, KRAS mutations are significantly more frequent in microsatellite stability tumors[9], while MSI-high cancers are characterized by BRAF mutations[10].
- KRAS mutation frequencies in various visceral metastases of colorectal cancer were also found to be significantly different. It suggesting that KRAS mutation status may affect the pattern of organ metastasis process.[11].
- The recent studies indicated that KRAS status of locoregional lymph node metastases were different from the primary in 31% of cases [145] suggesting a relatively frequent change during tumor progression[12].
- Considering the stringent criteria for accuracy of KRAS mutation testing (>97%), it is evident, that the reported frequencies of discordance of KRAS status between primary tumor and its metastasis (4-20%).
- Patients with KRAS-mutant in metastatic colorectal cancer (mCRC), typically presenting with right-sided tumors that are more aggressive on cancer recurrence.
- Mutations in KRAS genes of downstream effectors of EGFR signaling, such as KRAS, could explain resistance to anti-EGFR therapy.
- Patients are even harmed by therapies targeting EGFR, due to KRAS mutations[13&14].
- The National Comprehensive Cancer Network (NCCN) has a guideline for the KRAS mutation status determination in colorectal cancer stating that the diagnostic test can be performed either on the primary tumor tissue or on the metastatic.
- Furthermore, it is important to study and evaluate the mutations of other tumor suppressor genes or oncogenes related to the EGFR signaling pathway in colorectal cancer.
- Pylayeva-Gupta Y, et al., (2011 ). Nat Rev Cancer. 13(11): 761-74.
- Karnoub AE and Weinberg RA. (2008). Nat Rev Mol Cell Biol, 9(7):517-31.
- Yamauchi M, et al., (2012). Gut. 61(6): 847–54.
- Rosty C et al., (2013). Modern Pathology. 26(6):825–34.
- Burmer GC and Loeb LA (1989). Proceedings of the National Academy of Sciences of the United States of America. 86(7): 2403-7.
- Chang YY, ((2016). Am. J. Surg. 212, 537–544.e3.
- Valtorta E, (2013). Int. J. Cancer 133, 1259–1265.
- Jonsson M, (2009). BMC Clin. Pathol, 9, 8.
- Nash GM, et al., (2010). Ann. Surg. Oncol, 17(2), 416-424.
- Zlobec I, et al., (2009). Int. J. Cancer, 127(2); 367-380.
- Losi L, et al., (2004). Oncol. Rep, 12(6); 1221-1225.
- Baldus S, et al., (2010). Clin. Cancer Res, 16(3); 790-799.
- Gong J, et al., (2016). J. Gastrointest. Oncol, 7; 687–704.;
- Benson AB, et al, (2018). J. Natl. Compr. Canc. Netw. 16, 359–369.